|
|
International |
|
Overview |
|
|
International |
|
Overview |
Index of articles on this page
Global Aspects of Cardiothoracic Surgery, 2010
Global Expansion of Cardiac Surgery
in the New Millennium
A. Thomas Pezzella M.D.
(Asian Cardiovascular & Thoracic Annals 2001; 9:253-256)
Shortly after the submission of this editorial, a massive terrorist attack took place in the United States (US) on September II, 2001. This tragedy killed over 6,000 people and injured countless more both physically and emotionally. Many of those killed and injured were from other countries as well. Clearly, this has created inter-national outrage and has focused international awareness, fear, and concern for the whole problem of terrorism and what it represents. I think all of us in the cardiothoracic community are united in extending our sympathies and sorrow to the families, relatives, and friends so deeply affected by this immense tragedy. I have been personally moved by emails received from colleagues around the world expressing their condolences and support. Hopefully, it will bring us all closer together to work in a common effort to not only rid the world of terrorism, but to try and understand the conditions that spawned it, and ultimately come to the realization that we are all human beings sharing this fragile planet for such a short time. Perhaps by assisting others and fostering common goals and objectives, as I have tried to cover in this editorial, we are - in fact - helping ourselves as well.
Furthermore, medicine is one of the few spheres of human activity in which the purposes are unambiguously altruistic - in itself, a remarkable achievement.
With the advent of humanism during the Renaissance, medicine moved from the stagnant theories of the four bodily humors - blood, phlegm, yellow bile, and black bile - to a more focused understanding of human anatomy and physiology. The explosive expanded growth, however, came over the last two centuries with notable advances in chemistry, cellular biology, genetics, anesthesia, microbiology, body imaging, and pharmacology.
The challenges of the 21st century are numerous. Against the background of environmental, economic, political, cultural, and social problems, the role of medicine and healthcare has become increasingly more important and dominant, especially in terms of cost and access. The world population stands at 6 billion, with a growth to 9 billion by the mid-21st century. There were over 55 million deaths worldwide in 1999 (The World Health Report 2000, (
http://www.who.int/whr). Surprisingly, over 33 million were secondary to non-communicable conditions. Of these, approximately half were secondary to cardio- vascular disease. Ischemic heart disease accounted for over 7 million deaths, and rheumatic heart disease almost 400,000 deaths. Epidemiological transition is defined as a shifting of these chronic diseases to those countries and regions where there is improvement of social and economic forces. The emergence from famine, communicable disease, and pandemics to degenerative chronic disease has and will slowly occur.(2) This will place an increasing burden on the global healthcare system.With regards to heart disease, many of the transition countries and economies are still faced with the "first wave" of infectious etiology (e.g., rheumatic heart disease and Chagas' disease).
(3) As an example, the incidence of rheumatic fever remains one case per 1,000 children per year in Bangladesh. With a population of 120 million, the incidence is 20,000 new cases per year.(3) In a more recent survey in Yemen, the incidence was 3.6 per 1,000 (USA is 0.6 per 1,000).(4) At the same time, the incidence of Ischemic heart disease is rising in those developing countries where there is a rising lifespan, increased smoking, decreased infant mortality, and the unhealthy eating habits of Western society.(3)Faced with this background, the cardiac surgeon of the 21st century must reassess his/her role in this "global village." The phenomenal growth and development of cardiac surgery is clearly a product of the last half of the 20th century. Within a short span of the 21st century, the artificial heart, xeno-transplantation, and genetic remodeling and transfer will be realized. This expansion, however, will be experienced primarily in the industrialized developed countries and economies. In recent years, with the dramatic impact of the Internet, communication has linked the international cardiac surgery community. More and more cardiac surgeons are aware of "what's going on." The cardiothoracic Surgery Network (CTSNet), pioneered by Drs. Ferguson, Replogle, Greene, and others has made basic and new knowledge readily available.
(5) This transfer of knowledge is immediate, precise, and complete. The challenge of the Internet, however, is not to dehumanize the experience. Just as the doctor/patient relationship must be earned and nurtured, so too the relationship between medical colleagues. There is a tendency to think of "us" (i.e., those with the knowledge, experience, and resources) and "them" (i.e., those without the same). Paul Sergeant described the "Le Colloque Singulier" which stresses the equality between two partners of a relationships As this transfer of knowledge reaches an equilibrium, the quantitative disparity will dissipate and the qualitative phase of adjusting standardized databases and evidence-based paradigms will then dominate the Internet.The major cardiothoracic societies have broadened their efforts to extend both the body of membership and the annual medical meetings to the international community. Again, Eugene Baudet stresses the need for direct relationships amid the fear that major annual meetings could be replaced by virtual meetings, thus replacing the transfer of knowledge with technology devoid of human interaction.
(7) Additionally, the major cardiac surgery databases are now poised and ready to develop and expand an international database.(5),(8)The American Society for Thoracic Surgery (STS) and the European Association for Cardio-thoracic Surgery (EACTS) should be congratulated in this endeavor. Caution, however, should be applied to expanding databases to the regional and international levels. Again, Sergeant stresses the point that the ultimate goal of database collection is not just an epidemiological survey, but a benchmark to achieve quality control.
(6) However, quality control is a gradual process. It should not penalize or hinder the developing, struggling, or emerging programs. This would only hamper or hinder access to care as these new and struggling programs will become hesitant, timid, or in fact paranoid with regard to reporting their data.At the academic and training levels, bold new initiatives are taking place. The concept of regional centers of excellence provides a logical and cost-saving mechanism to achieve standardization and parity in educations and training. Clearly, the major training centers in Europe and North America cannot accommodate the increasing number of trainees at the doctor of medicine (MD) or allied health level. Richard Jonas has highlighted the recent political constraints in the US.
(9) New regulations in 1999 have limited the Educational Council for Foreign Medical Graduates (ECFMG) sponsorship for foreign medical graduates. Now rigid criteria and time restraints will be placed on non-accredited programs to obtain J1 visa (a training visa usually granted to physicians entering the US as residents or fellows) status for its fellows.In contrast, David Cheung has outlined a bold training program in China which can well serve as a model for other Asian countries.
(10) Additionally, there has been active growth in establishing regional centers of excellence in India. This has been sparked by a bold cooperation between industry and established cardiac centers. This is clearly an attractive strategy for large populations like China and India.Two recent addresses generated an increased awareness and interest in this global expansion. Hans Borst nicely and succinctly presented an organized approach of Western European centers to help their Eastern European and Russian colleagues.
(11) James Cox, in his presidential address at the recent STS meeting, presented a bold and challenging strategy to broaden and expand cardiac surgery globally. His recommendation of the utilization of regional Internet consultations and regional referral centers are certainly innovative and worth exploring. Financing these endeavors will require corporate and government support. This address will certainly spark off increased interest and initiatives, as well as debate and controversy.As we await the logical progression of the aforementioned areas, individual preparation is warranted. Just as cardiac surgeons prepare themselves for new procedures and operations, so too background knowledge and preparation is necessary and required to enter the "global village." For those individuals or groups attempting to get involved internationally, a few recommendations are humbly suggested as critical to any immediate, short-term, or long- term strategy, whether it is done at a local, personal level, or as part of a broad-based international initiative.
1. Any individual, group, society, corporate entity, quasi-government, nongovernmental organization/private voluntary organization, or governmental body must have a global perspective of geography, environmental issues, and political, economic, social, and cultural considerations of the nation or region of the world being considered. This information is readily available. Background information from the United Nations (UN), World Health Organization (WHO), International Monetary Fund (IMF), and World Bank is readily available on the Internet. The US State Department, as well as Brigham Young University (BYU), offer background notes on most countries. (189 countries - member nations of the UN.)
2. Knowledge of the past and present experiences of individuals and groups involved in international activity should be sought and studied. As an example, Children's Heart Link (
3. Cardiac surgery programs in developing countries or emerging countries can be categorized as follows:
a. Nonexistent, but wanting to start.
b. Previously existent, but failed.
c. Small or even larger existing programs now limited by financial and
political considerations.
d. Ready to start, but needs financial and political support.
e. Already functional, but needing academic support.
f. Various combinations of all the other examples.
4. Appreciation of the need to build and develop relationships. Just as in building any practice, it is important to have mutual trust and respect along with a sense of working in partnership. The traditional US approach of depositing money and material on the "port" without any involvement will not get the job done. Any relationship should be focused with attainable goals.
5. What is the role of the industrialized developed donor programs?
a. Provide and identify leadership in the host program and work
together in this partnership.
b. Develop the concept of mentoring rather than dictating. Mutual
collaboration is crucial. Many times, the developing program is the
teacher with a wealth of information and experience (e.g., technical
aspects of closed mitral commissurotomy).
c. Implement a managerial base that makes the strategies work.
d. Provide specific technical assistance, especially in the
infrastructure and biomedical areas.
e. Develop a strategy over time (usually 3 to 5 years) with specifics
that realize completion of the project.
6. What is the role of the developing host programs?
a. Provide the host program with basic information, i.e.,
infrastructure, background history, politics, and economics.
b. Develop a plan or strategy, i.e., what is to be accomplished, being
realistic regarding success or failure.
c. Facilitate arrival, departure, accommodation, and social program for
host group. Building a lasting friendship and future bridge of
co-operation.
d. Recognize that free or donated equipment and supplies are short-term
(usually 2 to 5 years). Thereafter, negotiations with government,
industry, and the private sector must occur to sustain the program.
7. Understanding the corporate role.
a. Their willingness to help in the short term with financial
support, donated goods, and services.
b. Recognize that they have financial constraints.
c. Being realistic regarding expectations from corporate sources.
8. An appreciation of language. English is the dominant medical language. Yet in the majority of the world population, it is at best a second language. John Benfield has beautifully and boldly outlined the importance of language and the need to communicate in English.
(13) For the normative speaking, an attempt must be made to acquire a working scientific knowledge of English. Native speaking individuals must show patience and understanding. At the local, up close, and personal level, any attempt to learn the native language - even a few phrases - will enhance and strengthen relationships.9. An appreciation and sensitivity of the ethics of medicine, particularly as it relates to clinical research. Research involving human subjects in developing countries is a major concern. A knowledge of the principles of the Declaration of Helsinki is essential. A sound research design and following basic ethical principles will yield research that is free from any debatable results.
(14)10. The concept of regional referral programs is sound, practical, and cost-effective. Yet, one must appreciate national pride and the hesitancy to refer patients to a neighboring country. Regional training centers are more feasible.
11. Sending or referring patients to the developed programs has been very effective, but of short-term benefit. Approximately 50 US programs have accepted indigent, non- paying, or non-access patients over the years. It certainly has benefited those selected individuals and has added hope to the rest. It also gives the host program an up close and personal insight into the problem. Yet, it is not cost-effective. Some organizations like Variety International and the Gift of Life program in metropolitan New York provide some financial support. Historically, paying patients from foreign countries have and continue to come to the large centers in the industrialized countries.
12. An appreciation of the other major healthcare concerns of the host country. Usually, the minister of health is faced with a small budget (less than 5% of the Gross Domestic Product) to provide for all the healthcare needs. The sophisticated and expensive curative side of medicine must be balanced with the less expensive, preventive side of medicine. A longitudinal approach to a disease like rheumatic heart disease, by emphasizing preventive strategies to control rheumatic fever as well as identifying and treating the problem, should be considered. Working with family planning and prenatal care programs also helps with trying to decrease the incidence of congenital heart disease. It may also be worthwhile to focus on low-risk congenital heart operations initially. A tremendous burden is placed on local healthcare personnel in triaging the enormous number of children with congenital heart defects.
Central to these recommendations is an appreciation of the concept of transfer. It is simply the geographic transfer of three basic entities from the industrialized nations and regions to the less developed or emerging nations and regions:
i. Ideas, knowledge, technology, logistics, planning, and strategy.
ii. People or personnel.
iii. Things, i.e., equipment and supplies - be they disposable or
non-disposable.
What facilitates or hinders this transfer is money and ego. Clearly, financial issues are key to the process. Yet not only the amount, but the most beneficial use of sparse funds, is crucial. 'Me quantity of money is not as important as spending it well. According to the WHO, the US spends $3,724 per person on healthcare each year. Yet it ranks 37th in the world in terms of quality of care. Ego refers to the personalities, biases, and misunderstandings, befuddled with bureaucracy that makes the process difficult and frustrating. A spirit of understanding and cooperation, tempered by patience and an open mind, will clearly facilitate the process.
It is my hope that more letters, editorials, and scientific articles are generated to debate, challenge, or support these concepts through the pages of the Asian Cardiovascular & Thoracic Annals. Finally, it must be stressed that the international growth of cardiac surgery still favors the developing world, and in tows troubled times the obstacles we all face in trying to assist colleagues have grown even more daunting. Challenges certainly worth undertaking for the good of all Mankind.
REFERENCES
Evolving
Global Approaches to Cardiothoracic Surgery
A. Thomas Pezzella, MD
(Posted 12/31/06)
Abstract
The incidence and prevalence of cardiovascular disease continues to increase globally, especially in emerging economies and developing countries. Cardiothoracic surgery also is growing, despite decreased access availability of surgical centers, and cost issues. The increase in incidence and prevalence of atherosclerotic coronary artery disease, rheumatic heart disease, congenital heart disease, trauma, and thoracic malignancies is a more urgent problem or challenge than realized in these emerging economies and developing countries. A determined focus and cooperation between the preventive and curative elements of core is warranted. This represents a paradigm shift of shorts to develop a consensus that brings together a team approach that includes prevention, promotion, diagnosis, treatment, and rehabilitation.
I keep six honest serving-men
(They taught me all I knew);
Their names are
What and Why and
When and How and Where and Who
Rudyard Kipling
Introduction
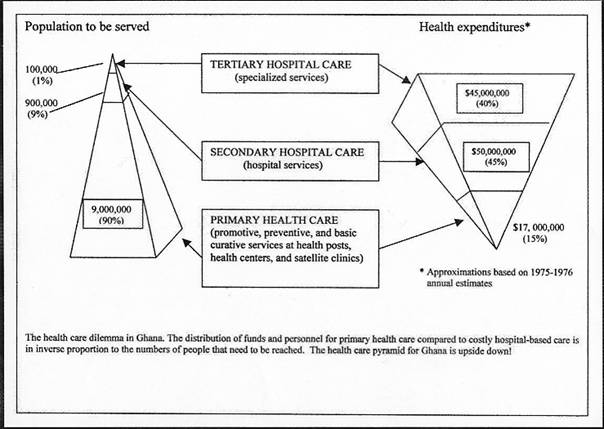
The world population stands at 6.5 billion people with an annual death rate of 57 million. Cardiovascular disease (CVD) remains the number one annual cause of mortality with more than 17 million deaths per year. These and other diseases of major concern to cardiothoracic surgeons are summarized in figure (1) 1, 2. The traditional individual approaches of preventive and curative strategies, though productive in the developed economies, have not had a major impact on reversing the overall trend. In fact, the incidence of cardiovascular disease continues to rise, in emerging economies. Clearly a new strategy or paradigm shift is warranted. This mandates increased cooperation between the preventive public health sector and the curative patient oriented sector. The product line or the cardiovascular disease specific approach encompasses prevention, promotion, diagnosis, treatment and rehabilitation. Strategic or organizational elements combine with tactical or managerial elements to build a consensus that is collaborative and not competitive or adversarial. The horizontal concept is nothing more than turning the flow of prevention or care from the pyramidal or vertical flow to a more practical mode where all aspects of health care are handled at the same time. All five elements are approached concomitantly, rather than the World War concept of attacking the beaches in waves. This horizontal flow of care is practical and cost effective. (Figure 2) Future models and trials will be necessary to test this hypothesis or paradigm shift i.e. a reorientation of thinking about this devastating problem or challenge. The traditional vertical or hierarchical pyramid model is no longer practical or cost effective. (Figure 3) 3 The more for less must compromise with the less for more concepts. Sub Saharan Africa (SSA) will be highlighted, since it represents the least served region of the world with regards to health care, especially cardiovascular disease. Background This world population of 6.5 billion people lives on 29.2% of the earth's surface, the remaining surface being covered with water. This population occupies 193 countries, 61 dependent areas, and 6 disputed territories. In contrast to the annual world mortality rate of over 57 million, there is an annual overall population growth rate of 1.14% or 80 million more people per year increase in overall world population. The global birth rate of 20-24 births/1000 population, and the death rate of 8.86 deaths/1000 population is almost double in SSA. The global life expectancy is 64.05 years compared with less than 51 years in SSA. 4, 5, 6 Further insight into SSA reveals that eight of the top ten countries with the highest infant mortality rate are in Africa. The human development index (HDI ) 7, which is an indicator of quality of life, again reveals that 27 of the top 30 countries in the world with the lowest HDI are also in Africa. HIV/AIDS infects 34-46 million people worldwide with 25.0-28.2 million cases in SSA. 2.2-2.4 million of the annual 3 million deaths secondary to HIV/AIDS are in SSA. The global prevalence rate of 0.9-1.3% is 7.5-8.5% in SSA. This background perspective is necessary as we develop the case for increased concern for non-communicable diseases, and try to strike a balance in priorities.
| * HDI – In 1990-1991 the United Nations established the Human Development Index that includes GDP or GDP per head, adult literacy, average years of schooling, and life expectancy Scaled 0-100, with >80 as high, 50-79 as medium, and <50 as low. |
The reasons for this disparity in SSA can be attributed to many causes. Simply stated the social, political, economic, environmental (geographic), and demographic factors (SPEED) are the basic elements. Unfortunately, government financing of education and health care are not high priority in most countries, but especially developing countries or emerging economies. (Figure 4) The debate between the Neo Malthusians who believe the growing world population is unsustainable and the Technocentrists who believe that emerging technologies can and will support a rising world population, continue to evoke a sustained emotional response. In summary, ego or the human factor, and money or economics play dominant roles in the overall approach to the challenge of improved, and equitable health care access, evaluation, and treatment.
Given this broad background of the global and the African example, let us focus further on the health statistics. Of the 57 million worldwide deaths in 2002, over 18 million were from communicable diseases, more than 33 million from non-communicable diseases, and over 5 million from injuries.8 A projection for 2005 is summarized in Figure 5 6. Of interest to Cardiothoracic/vascular (CTV) surgeons are the deaths attributable to cardiovascular disease (CVD), thoracic malignancies, and trauma. (Figure 1) Despite on overall decreased prevalence in SSA, the incidence of death from CVD rose from 8.15% in 1990 to 9.20% in 2000. This incidence continues to rise. Surprisingly violent trauma is less prevalent than blunt trauma. Road accident mortality in SSA is > 25/100,000 in contrast to 15/100,000 in the Americas. 8 Smoking, hypertension, stress, diet, and lifestyle changes will continue to impact on regions like SSA with a resultant increase in non-communicable diseases, especially ischemic heart disease, lung cancer, and trauma. It is estimated that over 80% of all CVD, cancer, and other chronic disease deaths in 2005 will occur in emerging economies6. What are the resources now present worldwide to deal with this present situation. Unger9, Cox10, 11, and Pezzella12 have summarized nicely the present situation, as well as proposing plausible strategies and recommendations. Briefly, there are over 1.5 million open-heart operations done each year worldwide by over 6,000 surgeons, in over 3,000 centers or units. Unfortunately only 2 billion of the world 6.5 billion population has access to these operations. There are 1222 open-heart operations per million population in North America, compared to 18 per million in Africa. This translates into 1 center per 120,000 people in the USA to 1 center per 33 million people in Africa. Strategic Initiatives| + Paradigm Shift - A term coined by Thomas Kuhn in 1962 in his book “The Structure of Scientific Revolution” (2nd edition, 1970, U. of Chicago Press, Chicago). “Scientific advancement is not evolutionary, but rather is a series of peaceful interludes punctuated by intellectually violent revolutions, and in those revolutions, one conceptual world view is replaced by another.” (www.taketheleap.com/define.html) |
Clinical
Most agree that the
incidence/prevalence of cardiothoracic diseases is increasing. Paying or
non-paying patients going abroad is of limited practical value, considering the
cost and the logistical difficulties - visa, housing, rehabilitation, and
uncoordinated, insufficient, or non-existent follow-up at home. Yet paying
patients will continue to go abroad for high cost, sophisticated care, until
such times that the local center(s) offers comparable quality care and
services. Not surprisingly, sophisticated cardiac surgeons and programs in some
countries like India are attracting paying patients to come to India for lower cost and state of the art care. Outsourcing is a growing business in
overall health care.
Regional referral centers offer a
better solution as a temporary or, even long-term situation. As an example,
there are several centers in South Africa that offer a model to study and
consider (Walter Sisulu Pediatric Cardiac Centre for Africa in Johannesburg and
the Christian Barnard Memorial Hospital in Cape Town). This may be a practical
solution for neighboring countries. It is recognized that most countries
eventually want their own program. Additionally, training for future programs
is within their scope of interest and influence. Also, it is easier to start an
adult program in places that are new or being upgraded. Pediatric procedures
are phased in progressively according to age, weight complexity, and
experience/development of the medical staff.
Education/Training
The internet, especially the www.ctsnet.org offers a wealth of information, skills, knowledge, and technology for the Cardiothoracic/vascular surgeon. At the humanitarian level the World Health Foundation www.world-heart.org has organized a website that will improve communication between individuals and NGO's (non-government organizations). This will facilitate sharing information with regards to needed programs or projects, resources, and thus matching these efforts in a collaborative way. In SSA developing a relationship with a foreign program, especially Europe is of practical value, as well as in neighboring countries with successful programs e.g. South Africa, Ghana, and Sudan. Outside of South Africa, there are no organized, standardized Cardiothoracic/vascular residency programs in SSA. A Pan-African initiative, like the Pan-African Society of Cardiology (PASC), may be a practical approach. Utilizing the knowledge of other African surgical societies like the West African College of Surgeons, and the Society of Cardiothoracic Surgery of South Africa can strengthen this unity and collaboration. The initiation of a dedicated journal, like the African Annals of Thoracic and Cardiovascular Surgery is another major step forward in stimulating clinical reporting of results and disseminating information amongst the African Cardiothoracic/vascular surgical community.
Research/Development
Certainly not a priority, but ultimately of major benefit and importance is the initiation of bench research, followed by clinical research. Foreign programs are showing an increased interest in research of diseases where there is a high prevalence e.g. HIV/ AIDS, malaria, rheumatic fever and tuberculosis.14 Establishing research centers in the area where the pathology is prevalent is both cost effective and practical. A word of caution is to establish strict guidelines according to internationally accepted standards, in recruiting clinical subjects.15 The Chain of Hope initiative at the Maputo Heart Institute in Mozambique is a notable example of this type of effort. (www.chainofhope.org)
Financial/Administrative/Political/Logistical
Multilateral agencies (United Nations; World Health Organization) are eager to develop collaborative strategies. Bilateral Agencies like the United States Agency for International Development (USAID) are working more with private voluntary agencies, as opposed to direct financial help to governments. Debt relief for emerging economies will provide needed short term relief, but health care is a low financial priority for most struggling economies. Non-government organizations (NGOs), also called Private Voluntary Organizations (PVOs) have been a major source of support. Yet this support is short term, usually 3-5 years. The private sector has enjoyed a healthy growth in some emerging economies eg. India. This is due, in large part, to a growing middle income group that can acquire private insurance, or self-pay. Overall bilateral foreign aid to emerging economies will not substantially increase over the insuring years. (Figure 6) A negligible share of that aid goes to health care initiatives. The United Nations in 2000 established the Millennium Project and issued the Millennium Development goals (Figure 7) 16. Unfortunately direct aid or goals for non-communicable diseases is not addressed. This project remains bogged down in strategy development, with a subsequent loss of time and money. This is highlighted by poor goal results at the 5 year assessment stage. As with many projects and initiatives more is accomplished with less financing by local, smaller groups and organizations. Targeting focused financial aid to these effects would pay much greater dividends.
A major problem in developing or emerging programs is the exodus of trained health care workers to developed programs. This "brain drain" is understandable on a personal level, but certainly not on a national or regional level. As an example, one-fourth of all physicians in the USA are international medical graduates.17 Nurse poaching is a severe problem, especially for Africa. This is especially true in South Africa.18 Training and retaining health care workers, especially doctors and nurses is crucial for overall health care planning, let alone cardiothoracic programs.
The host program(s) must have administrative and political support. This includes an organizational structure that minimizes bureaucracy, fraud, corruption and ego agendas. Foreign financial support, at best, is short term. Innovative, cost effective strategies with prudent management and attention to a disease oriented horizontal model may yield more effective long-term results.
The issue of product, i.e. equipment and supplies, be it disposable or non-disposable is another major problem. Donations are short term. Old donated equipment, or even newer equipment has problems insofar as preventive biomedical maintenance is concerned. Parts are a problem and equipment is frequently cannibalized to get needed parts. Logistical problems with customs and distributors also pose challenges. Inventory and organization is sorely needed in many programs. Ultimately the financial burden of obtaining the needed items for surgery falls on the patient and family since governmental or private insurance is unavailable or unattainable. Unfortunately, corruption at all levels not only drains financial sources, but has a major negative impact on all initiatives.
In summary, the challenge for the initiation and sustainment of Cardiothoracic/vascular surgical programs is a difficult, but attainable goal. Cooperation and collaboration should take priority over conflict and competition. It is easier to compete and develop incentives later when basic services are established. It is imperative that concerned physicians and health care workers consider the horizontal model. Gaining widespread attention to the problem of cardiovascular disease in emerging countries is crucial to gain public support, and access to the financial sources to start and sustain this effort. Teamwork remains the key ingredient to the success of this approach. Integration of a paradigm shift begins with the appreciation and realization that the present system can be improved and accelerated to meet this growing problem or challenge. Ultimately, a consensus can be achi8eved that approaches 4 problems or challenges (Figure 8):
(1) Equitable access to quality care, both preventive and curative.
(2) Affordability and cost-effective, recognizing that the major sources for financing are government, private insurance, or personal/family income.
(3) Sustainability i.e. strategies to continue financial and medical support to meet the increasing demand posed by aging populations, and increased non-communicable/chronic diseases, especially CVD.
(4) Accountability - Quality assurance, risk assessment, and database systems to insure transparency of the system for all to study, evaluate, criticize, improve, or reject.
The seemingly illusive goal to improve the quality and quantity of care for the patients we serve can be achieved
"You can accomplish anything in
life, provided that you
do not mind who gets the
credit."
Harry S. Truman
References
World Heart Report 2004. World Health Organization Statistical Annex p121-125.
Comment: Injury Surveillance is key to preventing injuries. Lancet 364:1564, 2004.
Hyder, AA, Morrow, RH. Chapter 1 - Disease Burden Measurement and Trends. In: Black, RE, Mills, AJ, ed. International Public Health, Gaithersburg, Maryland, Aspen Publishers. Merson, MN, 2001, p4.
Time Almanac 2005. Pearson Education, Inc. p. 553-554, p. 706-112.
World Fact Book - Central Intelligence Agency
http://www.cia.gov/cia publications/factbook/geos/xx.htm.
Fuster, V, Voute, J. MDGs: Chronic diseases are not on the agenda. Lancet 2005; 366:1512-1514.
The Economist - Pocket World in Figures, London, UK. Profile Books Ltd, 2006.
Mock C., Quansah, R., Krishnan, R., Arreula-Risa, C., Rivera, F.Strengthening the Prevention and Care of Injuries Worldwide. Lancet 2004; 363:2172-2179.
Unger, F. Worldwide Survey on Cardiac Interventions, 1995. Cor Europaeum (1999) 7:128-146.
Cox, JL Changing Boundaries. J. Thorac Cardiovasc Surg 2001; 122:413-418.
World Heart Foundation: Our Approach to Improving
Cardiac Surgical Services in Developing Countries
http://
www.world-heart.org/doc/8862
Pezzella A.T. International Cardiac Surgery: A Global Perspective Seminars in Thoracic and Cardiovasc Surgery 2002; 14:298-320.
Murray, C JL, Lopez, AD. Regional Patterns of Disability - free life expectancy and disability-adjusted life expectancy: Global Burden of Disease study. Lancet 1997; 349:1436-1442.
Yacoub, M. The Importance of Research at the Local Level in Developing Countries. American Association of Thoracic Surgery (AATS) 83rd Annual Meeting, Boston, MA, May 7, 2003.
Shapiro, H.T., Meslin, E.M. Ethical Issues in the Design and Conduct of Clinical Trials in Developing Countries. N. EngI J Med. 2001;345:139-141.
Sachs, JD, Mc Arthur, JW. The Millennium Project: a plan for meeting the Millennium Development Goals. Lancet 2005; 365:347-353.
McMahon, G.T. Coming to America - International Medical Graduates in the United States. N EngI J Med. 2004; 350:2435-2437.
Nelson, R. The Nurse Poachers. Lancet 2004; 364:1743-1744.
Figure 1
Selected Deaths by cause in WHO regions for 2002 (1)
| Total
Deaths 1) Cardiovascular diseases a) Ischemic Heart disease b) Rheumatic Heart disease c) Congenital heart abnormalities 2) Tuberculosis 3) Trachea/bronchus/lung cancers 4) Road traffic accidents 5) Esophageal cancer |
57,029,000 16,733,000 7,208,000 327,000 281,751 1,566,000 1,243,000 1,192,000 (2) 446,000 |
(1) World Health Report 2004 (www.who.int/whr/2004/annex/topic/en/annex2en.pdf)
(2) Comment: Injury Surveillance is Key to preventing injuries Lancet 364:1564, 2004
Figure 2
Horizontal Approach
|
Prevention/Promotion/Diagnosis/Treatment/Rehabilitation
Streaming Concept within a single institution, or multiple institutions within one geographic area
* Braithwaite, J. Goulston. Turning the health system 90°down under. Lancet 2004; 364:397-399.
|
Figure 3 (3)
Public Health/Preventive Focus Curative Care Focus
(3) Adapted from Hyder AA, Morrow, RH. Chapter 1 - Disease Burden Measurement and Trends. In: International Public Health, Gaithersburg , Maryland, Aspen Publishers Merson MH, Black, RE, Mills, AH, ed. 2001, p4
Figure 4
|
Health Indicators in E-9 Nations |
||||
|
Country |
Health Expenditures Per Person, 1990-98 |
Population, 2000 |
Gross National Product, 1998 |
% of GNP for Health Care * |
|
|
(dollars of purchasing power) |
(million) |
(billion dollars) |
|
|
United States |
4,121 |
276 |
7,903 |
12.9 |
|
Germany |
2,364 |
---- |
---- |
10.5 |
|
European Union |
---- |
375 |
8,312 |
---- |
|
Japan |
1,757 |
127 |
4,089 |
7.2 |
|
South Africa |
571 |
43 |
137 |
7.2 |
|
Brazil |
503 |
170 |
768 |
6.5 |
|
Russia |
404 |
145 |
332 |
4.6 |
|
China |
142 |
1,265 |
924 |
5.1 |
|
India |
73 |
1,002 |
427 |
5.4 |
|
Indonesia |
38 |
212 |
131 |
1.6 |
SOURCE: World Bank, World Development Indicators 2000 (Washington, DC: 2000), 90-92, 102-04, 106-08.
SOURCE: World Bank, World Development Indicators 2000 (Washington, DC: 2000), 10-12; Population Reference Bureau, “2000 World Population Data Sheet,” wall chart (Washington, DC: June 2000).
* The Economist – Pocket World in Figures. London, UK. Profile Books Ltd. 2003.
Figure 5
Projected global deaths by major causes, all ages, 2005 (6)
Figure 6
|
Development Assistance Contributions, Top 15 Countries and Total and 2000 |
||
|
|
2000 |
|
|
Country |
Total |
As Share of GNP |
|
|
(million 2000 dollars) |
(percent) |
|
Denmark |
1,664 |
1.06 |
|
Netherlands |
3,135 |
0.84 |
|
Sweden |
1,799 |
0.80 |
|
Norway |
1,264 |
0.80 |
|
Belgium |
820 |
0.36 |
|
Switzerland |
890 |
0.34 |
|
France |
4,105 |
0.32 |
|
United Kingdom |
4,501 |
0.32 |
|
Japan |
13,508 |
0.28 |
|
Germany |
5,030 |
0.27 |
|
Australia |
987 |
0.27 |
|
Canada |
1,744 |
0.25 |
|
Spain |
1,195 |
0.22 |
|
Italy |
1,376 |
0.13 |
|
United Stated |
9,955 |
0.10 |
|
All Countries |
53,737 |
0.22 |
Source: Organization for Economic Co-operation and Development (OECD), “ODA Steady in 2000; Other Flows Decline,” 12 December 2001; OECD, Development Assistance Committee, Development Assistance Committee Online, updated 30 January 2002; OECD, Development Assistance Committee, Development Co-operation 1993 (Paris: 1994), pp. 168-69.
Figure 7
|
Millennium Development Goals 15 1 Reduce extreme poverty and hunger by half relative to 1990 2 Achieve universal primary education 3 Promote gender equality and empowerment of women 4 Reduce child mortality by two-thirds relative to 1990 5 Improve maternal health, including reducing maternal mortality by three-quarters relative to 1990 6 Prevent the spread of HIV/AIDS, malaria, and other diseases 7 Ensure environmental sustainability 8 Develop a global partnership for development |
Figure 8
| Increase in overall quantity and quality of services |
Global Aspects of Cardiothoracic
Surgery, 2010
(400k PDF File)
![]()